Total Laparoscopic Hysterectomy
Total Laparoscopic Hysterectomy (TLH) is an advanced laparoscopic procedure. It involves removal of the uterus utilising keyhole surgery. Most people are aware that gall bladders used to be removed through a large incision and patients remained in hospital for almost a week after surgery. With the development of more advanced laparoscopic techniques, that operation is now seldom performed as most gall bladders are removed through keyhole surgery.
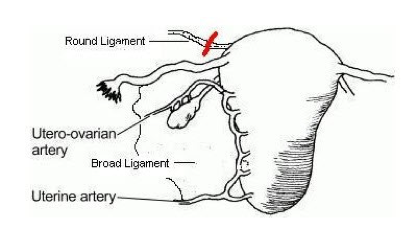
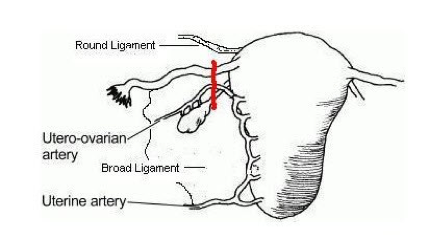
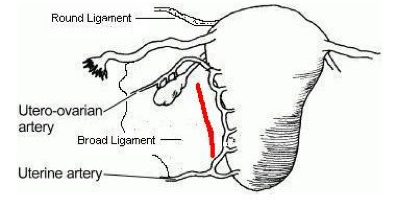
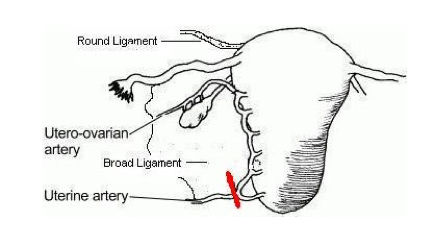
In many cases, Total Abdominal Hysterectomy can be replaced by a laparoscopic approach utilising 4 small incisions. Vaginal Hysterectomy, of course, does not require any incisions in the abdomen but is not suitable for many women who require surgery. If the uterus is enlarged, if there is no prolapse or the woman has not had a vaginal delivery then a vaginal hysterectomy is a more difficult operation. TLH allows full visualisation of the pelvis at the time of surgery and can change a difficult vaginal procedure into a safer operation. During a hysterectomy, the following structures are divided on each side of the uterus:
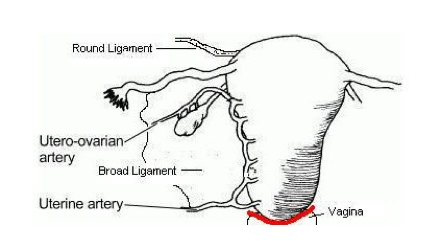
By incising this vaginal cuff, the cervix and uterus are finally freed from the surrounding structures, allowing the uterus to be removed through the vagina. A suture is then used to close the top of the vagina and reconstitute the attachment of the upper vagina to the uterosacral ligaments .

These structures are easily identified through the laparoscope.
At the end of the operation, the pelvis is checked for bleeding, then irrigated and a drain is placed through one of the small incisions on either side of the abdomen. This is used to remove excess fluid, gas and confirm that there is no new bleeding post-operatively.
Instruments: I have tried many of the different laparoscopic instruments available for this procedure. In my hands, I have found that the HARMONIC SCALPEL® is the most effective for dissection and division of the various tissues. A Bipolar forcep is used to coagulate (seal) the large uterine arteries near the level of the cervix. Because the HARMONIC SCALPEL® seals vessels at the same time as it cuts through tissue, blood loss is minimal and it allows for a shorter operative time. Short operative times decrease the risk of infection and deep vein thrombosis.
The HARMONIC SCALPEL® uses ultrasonic energy (vibration) for both precise cutting and controlled coagulation. Some important benefits include:
Minimal lateral thermal tissue damage
Minimal charring and desiccation
HARMONIC SCALPEL® technology reduces the need for ligatures with simultaneous cutting and coagulation
Fewer instrument exchanges simplify procedure steps
No electricity to or through the patient
Greater precision near vital structures
Minimal smoke for improved visibility in the surgical field
Post-Operative Recovery : Recovery from a laparoscopic procedure depends on what was done.
Diagnostic Laparoscopy: There are usually only two or possibly three port sites. Visualisation of the pelvis and abdominal cavity has been made, but there have been no incisions or excision performed. Most patients are able to be discharged the same day although 1 in 40 patients may need to stay because of nausea. Very occasionally a patient is unable to pass urine as a reflex response to pain. In this instance a catheter will be passed as a temporary measure.
Operative Laparoscopy: When procedures are carried out within the abdominal cavity via the laparoscopic technique, recovery may be delayed depending on the nature of the surgery. Any biopsy, division adhesions or more extensive surgery will be associated with some blood loss and this will irritate the peritoneal lining resulting in some inflammation and associated pain. Extended surgery time will lead to the trapping of gas under the diaphragm and this will give rise to pain in one or both shoulders. This gas will be reabsorbed within 24-48 hours. In addition to this, it is common for the bowel to become distended and so patients may experience abdominal bloating for a number of days following surgery. As with all surgery, pain at the site of all incisions is common, as will be some bruising. For major Laparoscopic procedures like TLH, patients have a drip which administers pain relief on -demand. This is called a patient-controlled analgesia because you just press a button and a defined amount of drug is administered. The drip and catheter (in the bladder) are removed the next morning. The drain is also removed at this time. This allows you to mobilise. Further pain relief is in the form of tablets or suppositories (bottom bullets) because pain is usually easily controlled at this time. Assuming all is well; patients are discharged the next day.
I am aware most patients can be discharged earlier, and I have done this. However, another day in hospital being cared for just ensures there are no issues left unresolved at discharge.